Architecting Trust:
Why Clinical-Grade RAG Architecture Fails in Clinical Environments?
⏱ 8–9 min read | 🏥 Healthcare AI & Clinical Innovation | 🎯 For Healthcare Leaders, Clinical Decision Makers & Professionals
Executive Summary: Clinical-Grade RAG Architecture
Clinical-Grade RAG Architecture or Generic “vector DB + LLM” Retrieval-Augmented Generation (RAG) patterns are not clinically trustworthy because they optimize for plausible language - not verifiable medical evidence.
In healthcare environments, architecture must enforce:
- Medical Entity Linking (UMLS-aware normalization)
- Attribution-first generation with zero-tolerance hallucination policy (AQA)
- Privacy-preserving, PHI-scoped retrieval
- Temporal reasoning and time-weighted ranking
The objective is not automation of diagnosis. The objective is Clinical Decision Support (CDS) for Clinical-Grade RAG Architecture that is evidence-grounded and auditable.
The Clinical Challenge: Clinical-Grade RAG Architecture
Clinical-Grade RAG Architecture documentation is heterogeneous and longitudinal. A single patient record may include:
- Structured billing codes (ICD-10, CPT)
- Problem lists
- Radiology narratives
- Discharge summaries
- Medication reconciliations
- Scanned PDFs
Even within one EHR, semantic consistency is not guaranteed. Generic RAG fails due to:
- Synonymy: “myocardial infarction” vs “heart attack”
- Abbreviation overload: “MS” (multiple sclerosis vs morphine sulfate)
- Negation complexity: “no evidence of pneumonia”
- Temporal drift: 2018 medication list vs 2024 reconciliation
In a consumer chatbot, hallucination is inconvenient.
In healthcare, it is a patient safety risk.
Therefore, Clinical-Grade RAG Architecture must be engineered as a CDS capability - supporting clinicians with evidence while preserving licensed medical accountability.
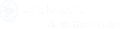
Figure 1. Clinical-grade RAG pipeline: MEL → temporal retrieval → attribution → verification → HITL
Technical Architecture (Risk-Averse by Design)
This architecture is intentionally conservative.
It is designed to support clinicians - not replace them
Pillar A
Medical Entity Linking (MEL) with Unified Medical Language System (UMLS)
Problem: Standard embeddings underperform in biomedical synonymy and abbreviation ambiguity.
Clinical-Grade Approach
- Extract problems, medications, labs
- Map mentions to UMLS CUIs
- Preserve original surface forms for auditability
Query normalization enables:
- Expansion (“heart attack” → myocardial infarction, MI)
- Constraint preservation (negation, temporality)
Result: Retrieval precision improves without sacrificing traceability.
The system remains CDS. Clinicians verify the cited source.
Pillar B
Hallucination Zero-Tolerance via Attributed Question Answering (AQA)
Healthcare cannot tolerate plausible guesses.
AQA reframes generation as attribution:
The model may state a clinical fact only if it can cite a supporting span.
Implementation Pattern
- Retrieve candidate evidence
- Generate answer with explicit citations
- Verify claim-level support against spans
Target metric:
- Increased claim support rate
- Controlled reduction in answer rate
In medicine, abstention is often safer than over-answering.
Pillar C
PHI-Aware Retrieval & Localized Vector Stores
Clinical text contains Protected Health Information (PHI).
Architecture must enforce:
- Patient-scoped retrieval
Role-Based Access Control (RBAC)
- Encrypted-at-rest indices
- Tenant isolation
- Audit logging
For CDS workflows, de-identification is often insufficient.
Access controls must be enforced pre-retrieval - not post-generation.
Deployment may be on-prem or within private VPC environments aligned with HIPAA compliance standards.
The system supports clinical workflows. Interpretation remains the responsibility of a licensed practitioner.
Pillar D
Temporal Context & Time-Weighted Retrieval
Clinical truth evolves over time.
Generic similarity search ignores recency.
Clinical-grade retrieval introduces:
- Timestamp decay functions
- Encounter-based bucketing
- Query-aware recency weighting
Example:
- “Current medications” → prioritize latest reconciliation
- “History of diabetes” → include longitudinal evidence
This ensures safer CDS behavior while preserving historical context.
Figure 2. Safety-first pillars for Medical RAG
Consumer RAG vs Clinical-Grade RAG Architecture
| Area | Consumer RAG | Medical RAG (Clinical-Grade) |
|---|---|---|
|
Cloud – First, Broad Indexing |
Patient – Scoped Retrieval, Private Vector Stores, RBAC, Audit |
|
Clinical trustworthiness increases with verification, even if latency & compute cost rise.
The Truth-Check Flow: Clinical-Grade RAG Architecture
Step 01
Retrieve & Constrain
- Validate patient scope
- Enforce access rights
- Hybrid retrieval (lexical + biomedical embeddings)
- Apply temporal weighting
Output: Ranked evidence set with metadata.
Step 02
Generate with Attribution
- Every claim must cite source + timestamp
- No diagnostic directives
- Evidence presentation only
Step 03
Verify & Decide
- Claim-level span verification
- Unsupported claims removed or downgraded
- Route to HITL if ambiguity persists
Output: Verified summary + audit bundle (citations, spans, confidence scores)
Figure 3. Trust vs latency trade-off in clinical RAG systems
Roadmap for HIPAA-Aligned Deployment: Clinical-Grade RAG Architecture
Phase 0
Governance
- Define CDS scope
- Establish escalation pathways
- Formalize change control
Phase 1
Secure Ingestion
- Normalize HL7 / FHIR / C-CDA
- Preserve provenance
- Attach metadata (patient, encounter, author, timestamp)
Phase 2
Clinical-Grade Retrieval
- Biomedical embeddings
- UMLS-aware MEL
- Hybrid + temporal ranking
- Cross-encoder reranking for high-risk queries
Phase 3
Attribution & Verification
- AQA enforcement
- Abstention policy
- Persistent audit bundle
Phase 4
Safety Monitoring
- Track faithfulness
- Monitor answer rate
- Evaluate retrieval sensitivity
- Clinical stakeholder review loops
Phase 5
Deployment
- Prefer on-prem or private VPC
- Encryption in transit & at rest
- Least-privilege IAM
- Vendor risk management
Conclusion: Clinical-Grade RAG Architecture
Clinical-Grade RAG Architecture systems optimize for fluency.
Clinical-Grade RAG Architecture systems optimize for verifiable truth, temporal correctness and patient safety.
For CMIOs and healthcare data architects, the decision is architectural - not experimental.
Trust in clinical AI is not a feature.
It is the outcome of deliberate design.
At Logassa, we engineer AI systems where reliability, compliance and auditability are foundational - not optional.
👉 The best time to start was yesterday. The second-best time is today-with Logassa Inc and our advanced AI solutions.
Know more about our works with our Blogs. Happy Reading!